
Back of the envelope scribbling on measles
Back of the envelope scribbling on measles

One of the things you get used to, when trying to understand things from public data is taking snippets and doing rough back-of-the envelope calculations on it.
In the early days of the measles outbreak, we had in Birmingham in England in Q4 2023, we got this.
This gives us enough for a back-of-the-envelope idea of how effective MMR vaccines are.
As with all of these calculations, the trick is to proceed carefully from one question: “What would we expect things look like if the vaccine did absolutely nothing?”
Now, what we really want is two groups which are alike in all relevant respects except that one had the vaccine and the other didn’t. If we had that, we could tease out the differences that the vaccine was driving, by looking at the differences from the situation where the vaccine did nothing. In the real world, outside a random controlled study, we never get this. We get two groups that are unlike in many ways: one of which is that one got the vaccine and the other didn’t. We then try to cope with as many of these other factors as we can, until we get a “good enough” answer.
The simplest1 place to start is to assume we’re looking at a random sample from the whole population. Then we look at the uptake of MMR vaccine across England (the rate for at least one dose is ~94%), and notice that we have found 198 cases in that 6% of unvaccinated population.
So if the vaccine did precisely nothing, we might expect to find a scaled number in the rest of the population: that is, we’d expect 198 * 94/6 = 3,102 cases in the vaccinated group.
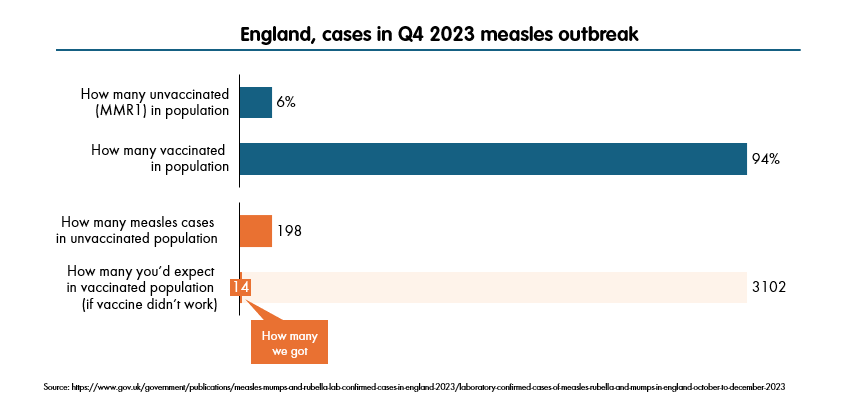
But we didn’t. We found 14.
So - assuming the only people the vaccine has an effect on, were those that have taken it - that is, the vaccinated group, then the only way we can be getting this is if that vaccine has some kind of “shrinking” effect on the number of cases.
We expected 3,102, we got 14. So - on this assumption that here we’re looking at a random sample from the population of England - the vaccine effect seems to have “shrunk” down the expected measles cases by a factor a 14/3102 = 0.005. To express effectiveness we take this number away from one: so a vaccine effectiveness vs symptomatic cases, of 99.5%.
Now in fact, in this case, we have oversimplified things quite a bit. We do not have a random sample. Most of the cases were in Birmingham, where uptake of MMR is much lower - nearer 90% than 94%. Also, we should make allowances for the fact that around 12% of the cases came in children under one year old, who are not able to have the vaccine in any case.2 Make these adjustments (i.e., exclude 12% of cases as occurring in <1 year old kids, and use lower uptake figures for Birmingham) and your effectiveness numbers come down a bit - you get to ~99% or a touch below.
Then you can further correct for the fact that measles tends to spread in small communities, and the vaccination rates at the below-local-authority level are likely to be even lower. These are not published unfortunately, but you can easily imagine that they’d get down to 80% or lower (you get these kind of figures in some places in London). And you can see how more careful work might end up close to the official figures of 95% rate for one dose of MMR (around 96% for two).3
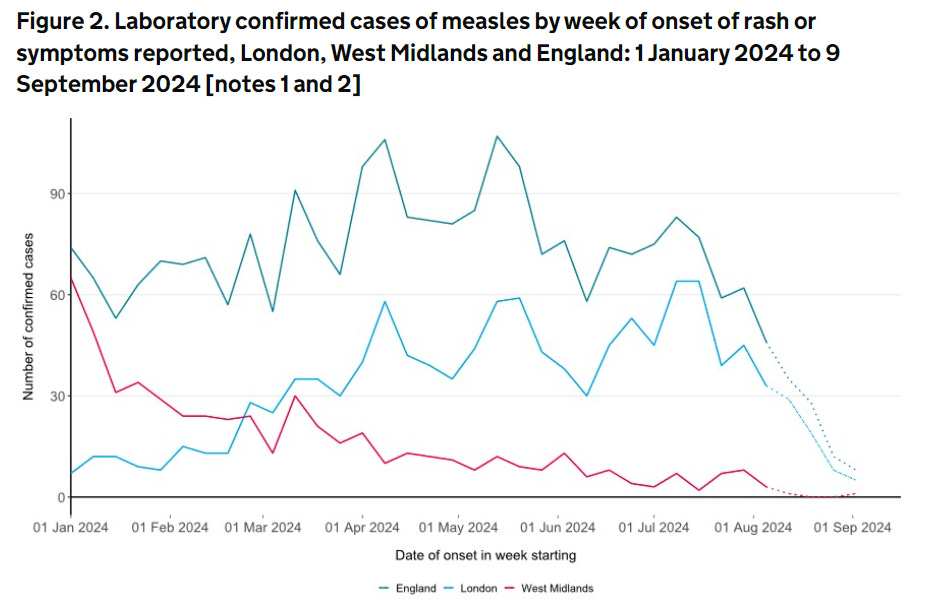
These extraordinary numbers - and implications for the sheer number of cases there would have been without the effect of the vaccines - are why everyone keeps going on about this particular outbreak being entirely preventable. It has now faded out in Birmingham, where it started but has crossed over to the even lower vaccination rates in London (Lambeth and Wandsworth in particular seem to be generating a steady stream of cases). This outbreak in turn has been somewhat suppressed over the summer, to around seven or eight new cases discovered each day, but measles is highly seasonal - it’s a winter virus.
So unless MMR rates have soared in the last few months, which is unlikely, then we are likely to hear more about this - and soon. In the meantime, we have a vaccine which appears to be living up to - or beyond - its “nameplate” 96% effectiveness, which confirms that our main (and - to be honest - only) serious line of defence, remains strong.
A bit over-simple in fact.
Though there is an effective maternal vaccine, which protects the kids in their first year of life. It has even lower uptake rates.
Obviously, these figures are the ones to use - there’s a reason I titled this “back of the envelope”