
Whooping cough - have UKHSA got the framing right?
Whooping cough - have UKHSA got the framing right?

The latest UKHSA press release on the resurgence of whooping cough is calm, measured, and careful to emphasise that while it might seem there a lot of cases, the disease is cyclical, so this sort of pattern is to be expected:
I.e., “Calm down. Don’t worry too much. It’s cyclical, nothing special about the UK here, it’s all countries, we’re just back in another cycle, perhaps with some extra lockdown effect”. And this tenor has been duly repeated in the press reports, which have been guided by the UKHSA’s press release and their expert quotes.
You get the same interpretation in the UKHSA’s recently updated monthly report, - which also calls back to an even bigger peak in 2012.
Usual seasonal patterns.
The thing is, this framing looks - to me at least - somewhat out of touch with the numbers.
In general, I am much against dramatising or exaggeration of any public health threats, and certainly against any artificial fear-based manipulation of public opinion. But in this case, I just can’t see how a “cyclical, business as usual, expected patterns” framing relates to reality.
Here’s the number of laboratory confirmed samples of causative agents, per week, including that last 2016 “cyclical” increase.
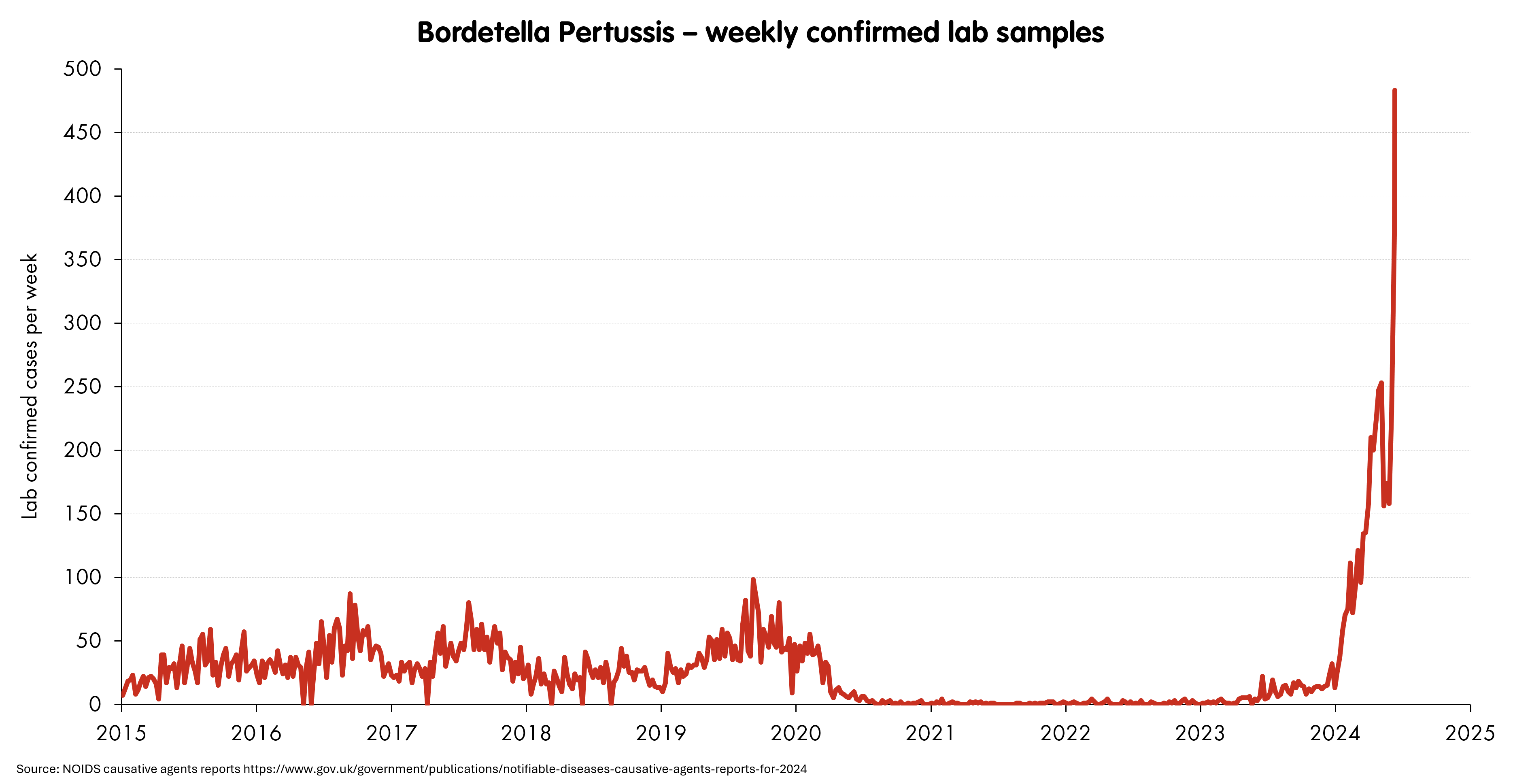
Now of course, unlike diseases like measles, whooping cough is instantly recognisable, even without a lab test for the causative agent. The “whoop” is so distinctive that experienced GPs can diagnose it over the phone (which in terms of infection control, seems like a pretty good idea). And not all of these may have bothered sending a sample to a lab - so maybe these numbers do not track outbreaks very well.
But whooping cough is a legally notifiable disease: any medical professional who diagnoses it is under a legal obligation to notify a central authority. So if you use those, much higher numbers (i.e., including all GP diagnoses with or without lab test), then you see a similar result. There were 4,534 cases reported over the whole of that last “cyclical year” 2016, and 6,557 over the “peak year” of 2012. We’ve only had 23 weeks of 2024 so far, and the total number of notifications is already 16,988. The most recent year I can find where that kind of run-rate is evident was 1986.
This would all be relatively unimportant if whooping cough was not particularly serious. But it is. It kills young children.
At the time of writing, the cases reported from January to April 2024 have resulted in the eight deaths - all (I believe) - of children under one year old. That was from the ~4,800 cases reported and lab-confirmed up to that point (a rough overall CFR of 0.2% - but note this is much, much higher in children under one year, and higher still in those less than three months old). Given the increase since then, we’ve seen nearly the same number of cases in May and June already, so - just going by some grim ratios - it seems likely that deaths: all of very, very small children in the first few months of their lives, are firmly in the double figures now.
So, I guess I’m putting this out there so that people can tell me what I’ve got wrong: the UKHSA framing of “it’s cyclical, don’t worry, we saw it in 2016, it was worse in 2012, it’s just normal”, seems just … well … massively wrong. The current spike looks new and unique in the last several decades; about as far from a cyclical effect as you can get.1
Now, I may be missing something here.2 NOIDS figures are tricky, and reporting delays makes things difficult to interpret, but to me, this whooping cough outbreak looks like something not cyclical, something that seems to be killing a lot of kids, and only “expected” to the extent that the falling childhood vaccination rates might have made us fear that a spike was on its way. With the added implication, of course, that these deaths were easily preventable, and future ones can still be prevented.
A big reason for such a lot of serious illness and death - and I’m a little tired of beating around the bush here - is the falling vaccination rates for both mothers and kids. The current vaccines are highly protective versus serious illness, while being less effective versus infection and transmission of the causative bacteria from child to child. So, while we’re not talking about something like measles, where you can achieve strong herd immunity in the population and stop transmission altogether, the vaccine will stop kids getting seriously ill. The vaccine given to mothers during pregnancy is especially important, as it protects the child in the first few months of life when they are most vulnerable to the disease.
If anyone reading this can point out what I’ve done wrong or misunderstood, please do let me know. The data is fragmented, the offset between the reporting-by-date-of-sample vs date-of-reporting tells of a significant backlog, which might be obscuring the true picture, and I’m only an amateur. If I’m reading the numbers right, then I’m totally bewildered by the “it’s cyclical, it’s no big deal” communication that has been going on from UKHSA and all quarters for months, with no sign of changing. So one obvious explanation is simply that I’ve screwed up - let me know if I have.
The sentence "The impact of the pandemic also means there is reduced immunity in the population" doesn't feel quite right to me. It sensibly implies that less people are immune than should be, but doesn't explain why. Looking at the spike, immunity is considerably reduced.
It's more than delayed cases.
It looks like vaccine avoidance or hesitancy, which was not present in previous cycles.
Almost as if people had been going around disinforming that vaccines are dangerous or something, when we know they are much safer than the disease itself 🤔
People will continue to be harmed until we have better controls and penalties for disinformation.
I don't like: “it’s cyclical, don’t worry, we saw it in 2016, it’s happening everywhere” as it makes it sounds like there is nothing that can be done, but clearly higher vaccination rates would reduce the peak of the next cycle. However it MAY be too late for vaccination to make any difference to this cycle, I don't know how long it takes from 1st dose to give a good reduction in transmission and how long the peaks of these cycles last.
There must be data from other countries that indicates how large the peak will be with the vaccination rates we had over the last few years, but I have not seen anyone discussing it. The medical people I expect would be sending out blog posts if they considered this to be a significant issues are not, maybe they know something we don't. Maybe vaccination have already returned to a high enough level to prevent the next peak and we are seeing the effect of unvaccinated children spreading to babies who are too young to be protected by vaccination. (There was a reduction in vaccination rates of babies in the Covid year.)
I expect they also don't want anything that will reduce the focus on catchup MMR vaccinations and are considering how best to use limited resources.