
Is COVID now just another winter virus?
Is COVID now just another winter virus?

It’s certainly closer than it was.
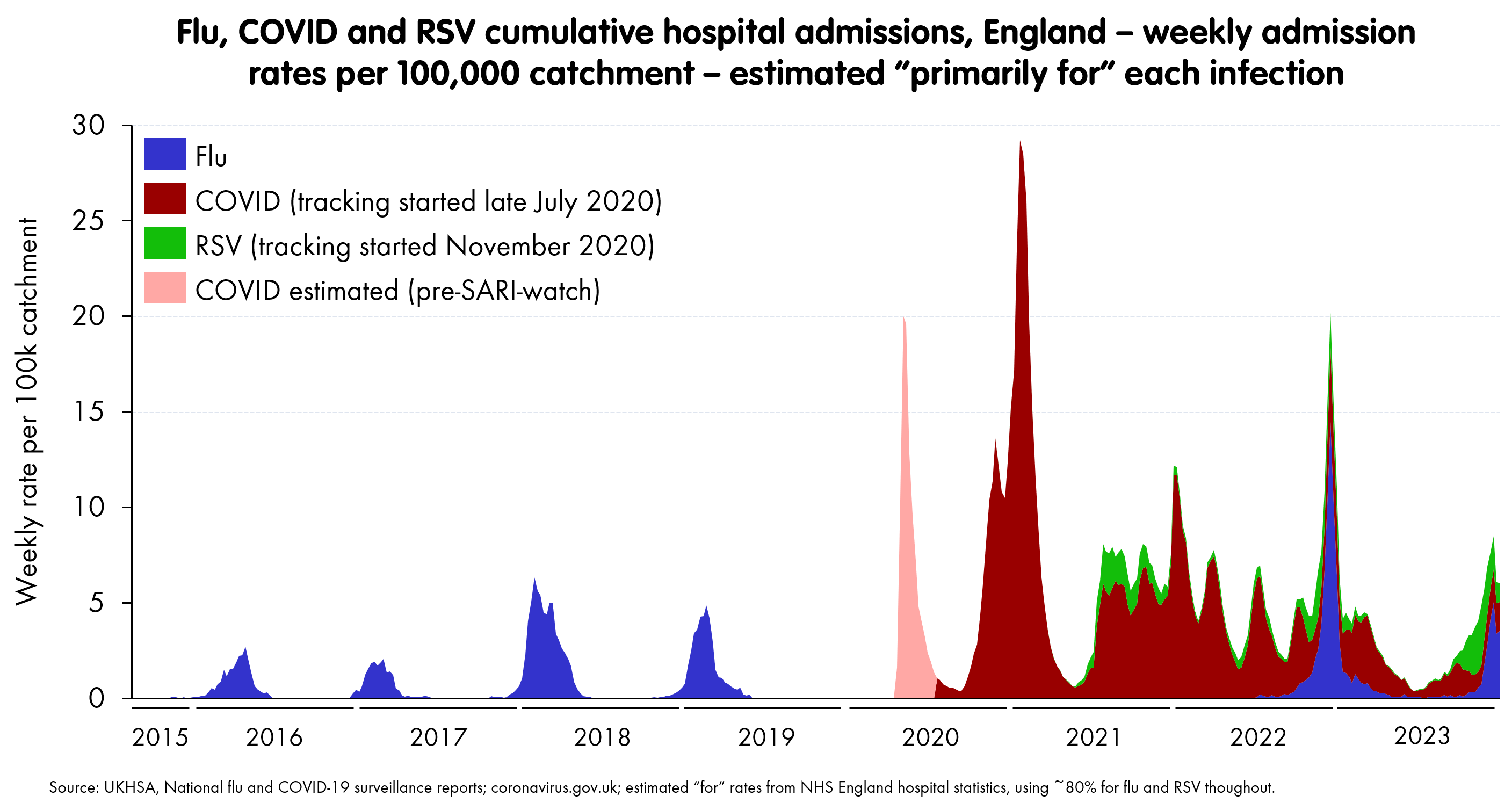
In hospitalisation terms - i.e., a direct pressure on the NHS - then we can use SARI-watch data plot its transition from its spectacular arrival in the UK to its current state, along with the previous few years’ flu waves.1

We can do the same thing for ICU admissions - though here the time period is a bit shorter, and we don’t have RSV (paediatric ICU seems to be treated differently in NHS data management). Again, I’ve estimated the first COVID spike from the dashboard.
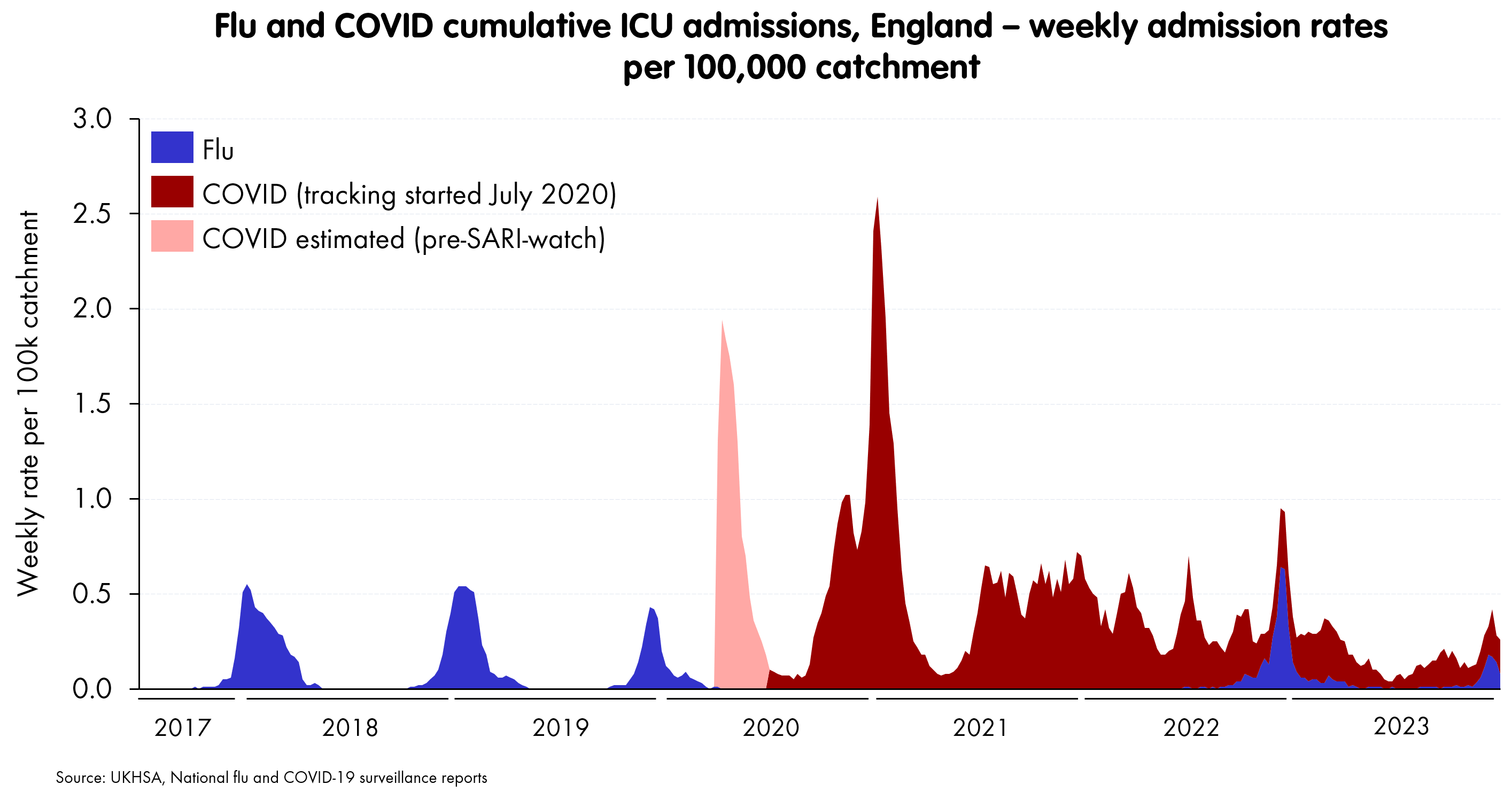
Now despite the fact that some of these lines (especially flu) may be somewhat underestimated throughout, due to patchier testing, or have varying degrees of ascertainment (COVID) this still gives a pretty useful view of a few points:
The sheer scale of unvaccinated COVID waves vs previous flu seasonal waves
The scale of winter 2022/3’s combined peak, which was only beaten in cumulative terms by 2020/2021’s pure COVID.
Towards the end, an alignment of these three major respiratory illnesses into winter peaks, which tend to be awkwardly simultaneous
It looks like COVID is taking a place alongside flu and RSV as a respiratory illness that peaks mostly in winter and combines with the other two to impose spikes of admissions, which put intense pressure on NHS capacity.
Another virus, sure - “just” or “just winter”?
Perhaps “just” isn’t quite the word. The combined peaks we’re now getting are considerably larger than anything we used to face - at least outside the very worst flu years. As a result, a fragile NHS is struggling to cope each winter.
In addition, we are still getting smaller waves outside the peak winter months, though these tend to be COVID alone. And - especially in 2021 and 2022, these started contributing to what NHS workers started calling the “eternal winter”. These dropped off in 2022, but there were still significant waves outside of the Dec-Feb winter window.
Again, we should be careful not to overstate these. After 2022, about 1/3 (best-efforts) are admissions primarily for COVID, as opposed to people who are admitted for other complaints, but also testing positive for COVID. So - arguably - you can reduce the red area by a fair amount, starting in 2022. Flu and RSV tend to be targeted tests and diagnoses, so although I haven’t any data, I shall assume similar pre-2022 rates throughout. If you apply these, you get this as my “best efforts” impression of the “for” the infection in question.2
And this brings us to a level where - again, arguably - a well-funded, functional NHS should be able to cope. The NHS we have is not coping, but this is at least as much down to the state of NHS as the virus.
Hospitalisation is not the only thing
And, of course, there are other worries about a novel virus coming in and infecting a large part of the population repeatedly (I’ve seen a credible estimate of an average infection for each person about once every 18 months - a mean which obviously conceals a great deal of important variation).
The most obvious is long COVID - the persistence of a variety of debilitating health effects long after the acute phase is over. It’s not at all clear (yet) whether this is a post-viral syndrome comparable to others, but has been thrust into prominence because so many people had COVID (and had it badly, which seems to be associated with the worst manifestations of long COVID). Whether it’s that, or there’s something about COVID that makes long-term effects particular widespread and serious, it’s worth taking very seriously indeed.
Predictions are hard - particularly about the future
Another obvious characteristic of COVID is its continued evolution, and - given it is so new - it could have plenty of potential to mutate into either a more transmissible, immune-evading, or serious illness. Flu and RSV could do the same of course, but the difference is that they’ve had a good long time to try at it, and so (we think) we know roughly the range they’re capable of. There’s much more uncertainty about COVID, and a jump like Omicron certainly took everyone by surprise.
So - another winter virus?
In terms of pressure on the NHS, I think that unless something new happens, then we can give a qualified “yes”, and endure the inevitable shouting. COVID is not currently driving waves capable of overwhelming the NHS on its own - it needs considerable help from flu or another infection to do that. And it will be managed similarly to other winter viruses. That is, there are likely to be autumn vaccination programmes (along with flu) for the most vulnerable to blunt the impact of the expected December-February waves, when a lot of people will be made seriously ill and die from it. And in those terms, it is comparable to flu.
In wider terms, in terms of long-term health effects, future mutations and so on, it’s pretty clear that COVID should still be thought of differently, simply because it’s so new and infections are so widespread. We don’t have a good understanding of how the long-term effects work, though it appears clear that the bulk of the worst long COVID cases were triggered by serious infections in the first, pre-vaccine waves. And we haven’t yet the experience we have of flu and RSV of how the long-term evolution will go - there’s just many more things that evolution can try out to surprise us.
I’ve estimated the first spike in April 2020 from the dashboard data. SARI-watch didn’t start clocking it until late July. I’ve not corrected it for the very obvious undercount - arguably, given excess deaths data - it should be similar to the second spike.
Since NHS England gives a “best efforts” rate for COVID, we can be relatively confident on these rates. For flu and RSV, I’ve chosen them to match a pre-2022 COVID rate of 80% throughout. Other than that, the biggest issue here is timing. The drop in “for” is associated with people in hospital. The rates are for admissions. These will usually track with a bit of a delay, but the relative magnitude of the first Omicron spike (Dec/Jan 2021/22 is massively affected by the timing offset). I suspect it is too high.