
Mixed messages: Trying to make sense of measles
Mixed messages: Trying to make sense of measles

Last week, I wrote something about how the measles situation may have looked OK since the Birmingham outbreak at the start of the year, but that even the partial and unreliable view we had into the underlying dynamics suggested “seeding” in the rest of the country - so to expect further bad news.
A few days later, there was further bad news.
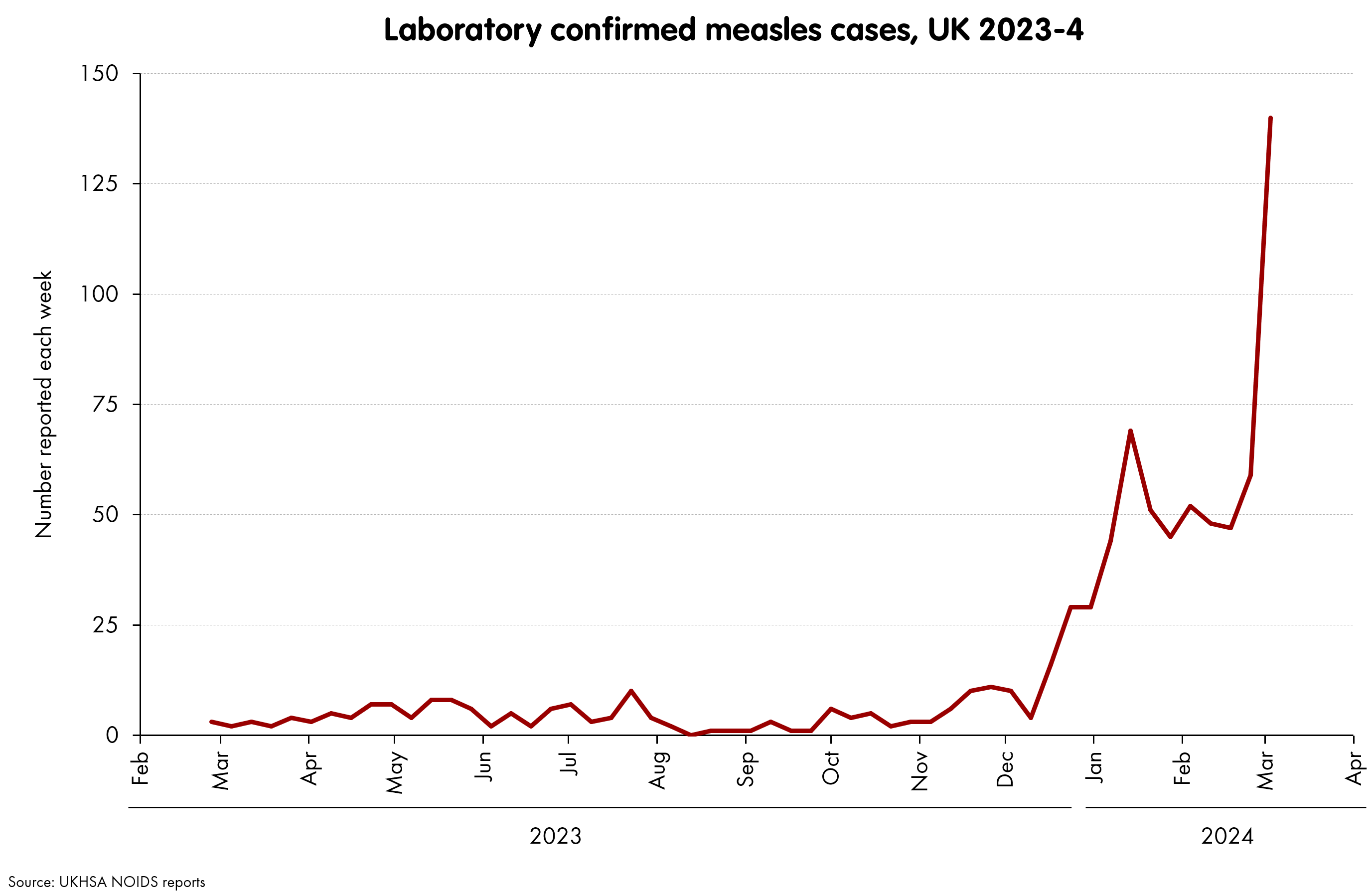
These lab confirmed reports are the ones for definitely-real measles cases, so this is the time-series to keep an eye on. However, there’s another one, which is more timely and more detailed in terms of location. These are statutory reports that doctors are obliged to submit when a measles case is suspected.
If I had been asked to make a prediction (shockingly, no-one asked), I would have said something like: “I think reports will be noisy, but would expect them to jump in London and the North West this week, as these seeding events start to get established”.
Numbers just came out for Week 9 (week ending 3 March). Is that what happened?
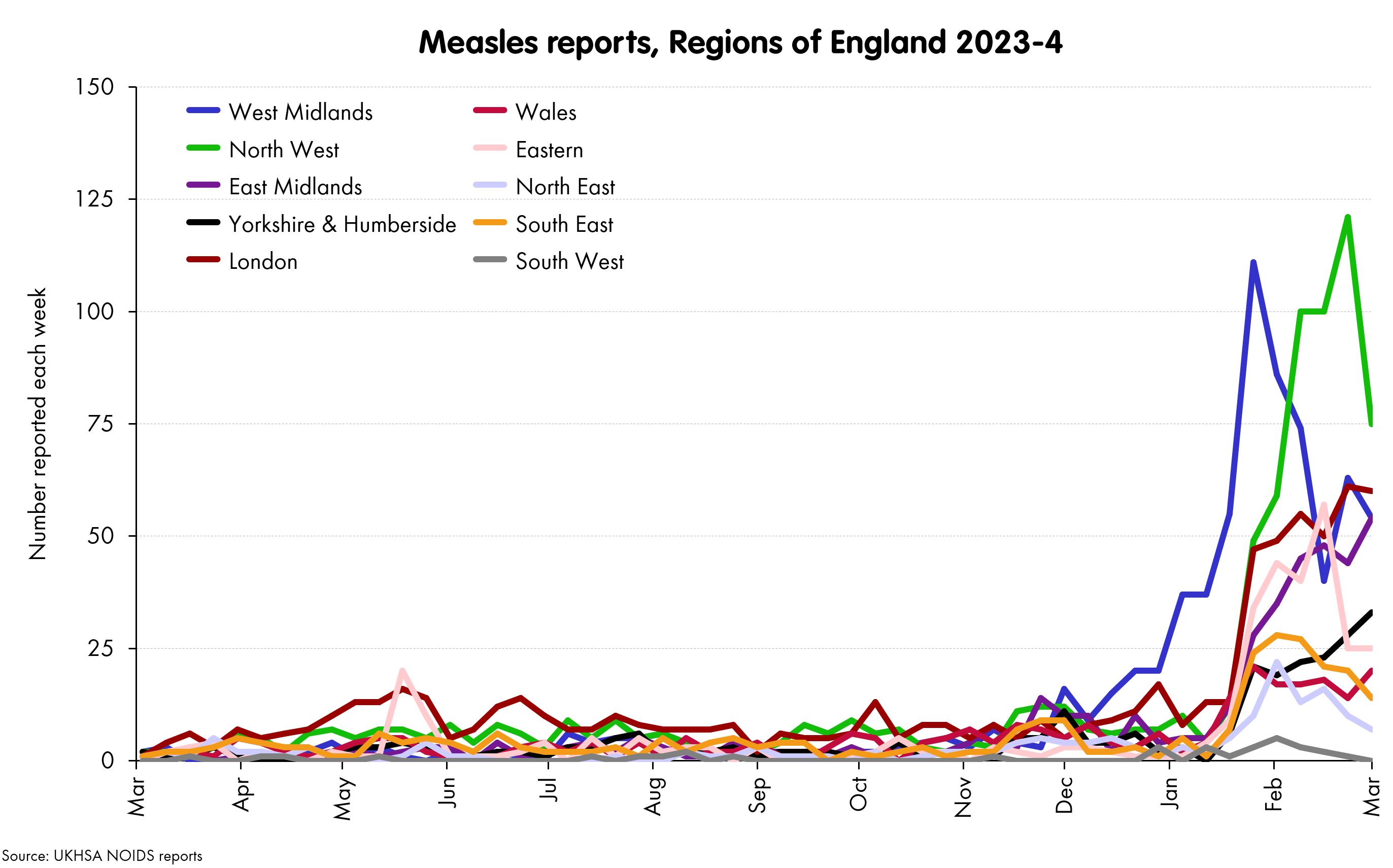
So no, it isn’t really. The North West and London are indeed now the highest regions in terms of reports, but if we had the sort of seeding events that were signalled by the lab reports, I was expecting more from both of them. These reports are not indicating that the spread is following the pattern I’ve been suggesting - at least not cleanly.
Before looking at possible reasons, one thing to point out. We should recognise the existence of a “reporting delay” effect, where the most recent week tends to get “topped up” as more reports come trickling in and assigned to those weeks. Fortunately - at least according to recent history- this does not seem a long-term effect: at a total level we have seen about 10-20% added one week later, but after that, they tend to be >95% complete. So on the above, it’d be reasonable to mentally add about 10-20% to the last points, but keep the others about the same. This makes a bit of a difference (London reports are probably still rising for example) but does not radically change the picture.
So, what do we think is going on?
I think we have three main possibilities:
It’s spreading but not being reported: there are more cases out there, but they are in communities that are hesitant to come forward and report, at least not until patients get properly ill.
It’s spreading and is being reported, but not yet: more reports will come in next week, as the (real) spread continues, especially in London and the North West
It’s not spreading: the striking jump in lab reports is hangover from the Birmingham outbreak, and is some combination of a backlog of cases being processed, and a much larger number of tests being done.
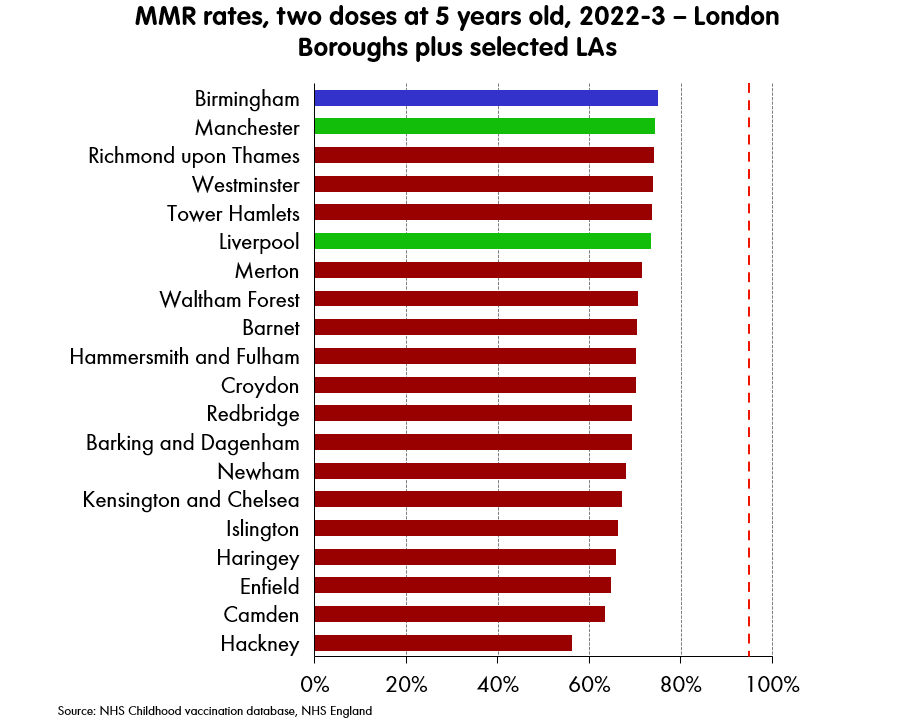
In support of #1, we could point to the vaccination statistics as split by ethnic origin, which show a rather striking picture.
If measles is - as you’d expect - spreading fast amongst under-vaccinated groups, the reasons behind that vaccine hesitancy might also delay approaching a GP or other medical professional, where a report of a notifiable disease could take place.

This of course would be very bad. If measles is spreading undetected, there’s not much that can be done to stop it (reminder R = 15 or so).
In support of #2, one could point to the last “jump” we saw in lab reported cases came a week or so before the jump in reports. Whatever mechanism is going on here (reporting mechanisms or timings etc), it seems that one might expect a larger jump in reports to come in not this week, but over the next few … when it can be dramatic.1

In support of #3, I have no support, expect the general rule that you should very much understand how a data sequence is generated (e.g., typical and variance in delays between collecting a sample and testing, how backlog numbers are dealt with, and so on.) UKHSA are warning on their NOIDS database of an issue with scarlet fever reporting, but not with measles. However, I only have a very little understanding of this, so there is indeed a chance that this jump to 140/week is an illusion, and in fact reflects not any underlying rise, but instead some reporting issues.
I doubt it though. If it is, I’d really like UKHSA to spell it out.
As a result, my money would be on some combination of #1 and #2. But I am honestly not too concerned with what the statutory notification numbers do in their own right: only about a fifth or sixth of them really turn out to measles.
What we should care about is the lab-confirmed number and what it does next.
If it continues to rise, then we are experiencing simultaneously:
a) The inevitable consequences of our actions, and
b) Some bad luck.
The inevitable part comes from allowing MMR rates to sink the level they are at now, particularly in large cities and particularly in London.
These kind of rates mean a significant measles outbreak - one large enough to damage the health of many people (including measles’ nasty trick of wiping out immune memory, which is something to watch with COVID around everywhere, and a combination of vaccination and prior immunity keeping it in check). Also large enough for measles’ other charming trick, which is to kill kids. It has a age-fatality rate profile that goes the other way round to COVID’s: it’s much worse for young children
The bad luck part is that inevitable consequence is happening already. Rates have been declining for a while, but the last time we had pockets anything like this (after the Wakefield fraud in 1998), we had 14 years before the Swansea outbreak in 2021. Timings are difficult to match, but it looks as though we have barely had half that time.
Whether this breaks out to a larger scale or not, if you are in any doubt at all as to whether you or anyone in your family are up to date on your measles vaccine, it is very, very worth going to your GP for advice.
I’ll leave it with the footnotes on the UKHSA’s time series of cases and deaths from measles 1940-2020, where they go into depth on the twenty or so measles deaths recorded in the UK from 2000-2020.

Visually, it looks like these datasets could also be consistent with a 6 week delay between the two reads. I don’t think these are plausible dynamics. First, it would imply that for the first time, there were zero false reports of measles in December 2023, and they were all real. More fundamentally, a measles PCR test has a 3 day turnaround, and I can’t see how it could be acceptable to have such a long delay in logging a notifiable disease.