

Twin Peaks - January 2024
Fire walk with me

An unwelcome arrival
Flu’s on its way.
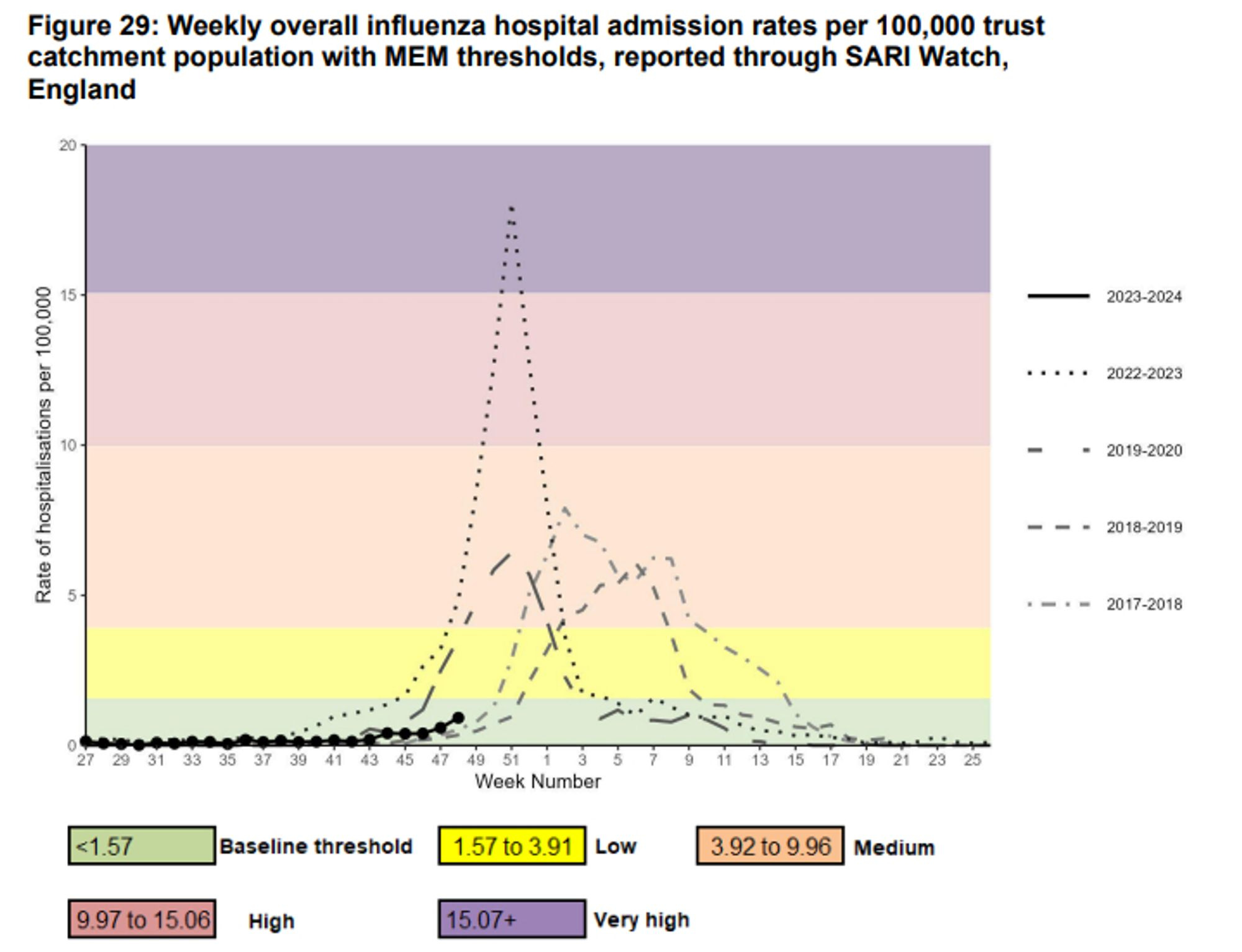
I guess it was too much to hope that it’d stay away all winter.
To make this trend clearer, let’s replot this data (or rather, data extracted from the above chart in the UKHSA’s flu surveillance reports) onto some log axes (exponential rates become straight lines).
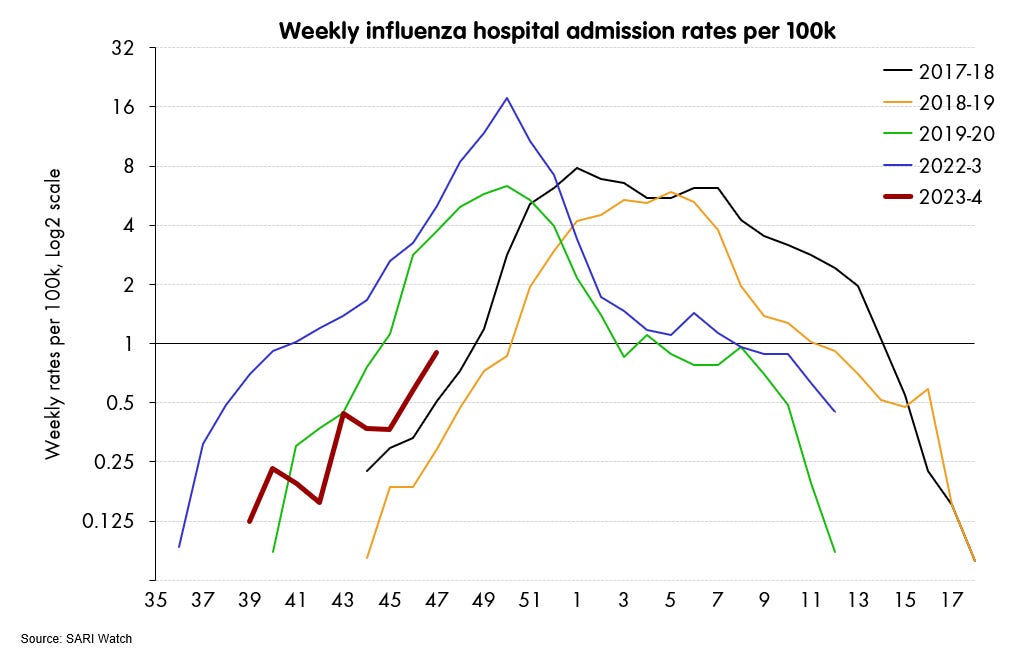
While the height of the flu peak is difficult/impossible to predict (flu is a notoriously tricky thing), but on its timing, we can see from past years that there is a pretty clear relationship between when the wave starts kicking upwards and when it peaks. And it looks like we’re roughly on for a peak around week 1 or 2. Maybe a week either side? January 2024.
A COVID surge is on its way
A flu wave pretty much normal, and pretty much on time, but now let’s add another chart.
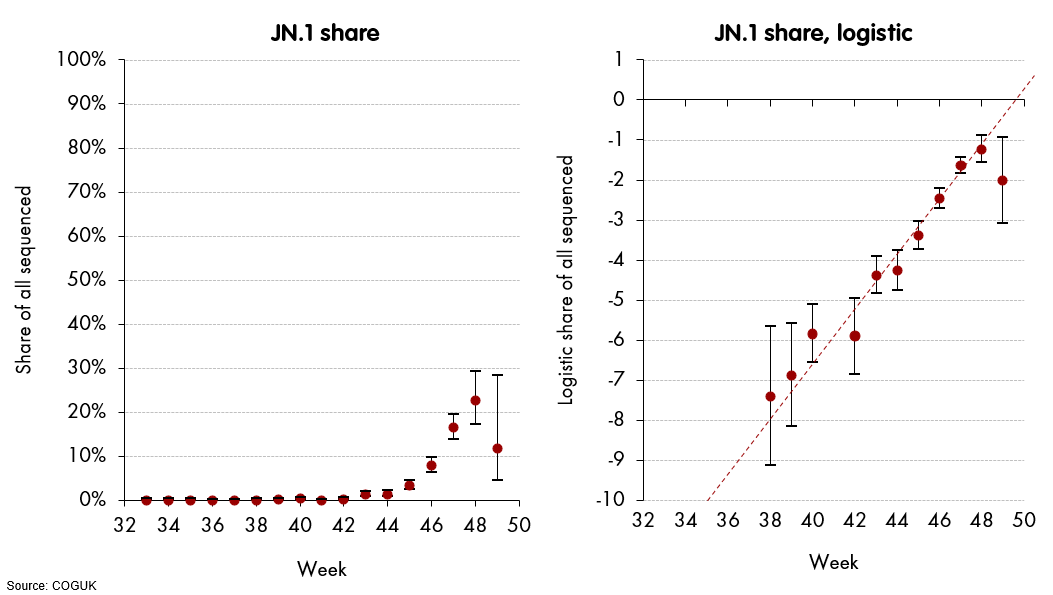
This one is for shares of JN.1 - the variant which, it’s increasingly clear, is the current candidate out of the COVID variants with relative growth advantage big enough to cause a significant wave in the UK.1

That is, JN.1 will be reach the 30-50% share range this week, and then its higher growth rate will dominate the overall dynamics of COVID from now onwards. Indeed, last week, we already saw hospitalisation rates turn around, when JN.1 represented 30% or less of the total.

Now, it’s mostly a guess how long any COVID wave lasts, though there is a loose relationship to the relative growth advantage of the driving variant. Looking at previous waves of a similar type, it seems likely that it will be going up for least four weeks.
Given where we are at the moment, and using some estimated relative growth numbers, a back of an envelope gets you around 1000 admissions/day for COVID by the second week in January. We haven’t seen that for a bit.
So, it seems disconcertingly likely that the last two weeks of December 2023 will see the upswing of simultaneous flu and COVID waves, both reaching their higher - possibly, peak - levels in the first half of January 2024.2
This is unpleasantly similar last year, where not only flu and COVID, but also RSV too, all peaked, nearly simultaneously, around the last two weeks of December (just by luck, this was the window in which the ONS pilot study was looking at all of them).

So, it looks like this year could be similar, just shifted back by two weeks, to January rather than December.
This is of course a bad situation to look forward to. Last year, emergency medicine pretty much collapsed for those couple of weeks. There was simply not space in the system to move people through the hospitals, and ambulances queued for hours at the front door. This is already starting this year (as measured by ambulance delays and trusts declaring incidents), and adding a double whammy of flu and COVID waves would most likely give a very similar result.
It looks pretty bleak in fact. And I’d certainly advise anyone in the UK that they should not plan in any accident or emergency medical episodes for January 2024.
Some cope
So, let’s look at some reasons to hope/cope that the outlook for January 2024 in the NHS might not be quite so bleak as it looks.
Flu is unlikely to be as intense as it was last year. It went up like a rocket, to levels we had not seen for years. Fortunately, it came down very quickly too, but the pressure in those few weeks was intense. It’s likely to be more “normal” this time. [I think this is correct and important]
RSV has (probably) already peaked - so it’s two out of three, not all three respiratory waves at once, like last year [I think this is correct and fairly important]


It’s quite likely that infection-hospitalisation rates for COVID are lower than they were, and even lower than last year. So the COVID wave may well have less impact than we would naively think [I think this is correct, but the levels of infection are already fairly high, so this nets out as a wash]
The very latest week of data gives a hint that JN.1 might be losing steam - the very latest share point is a lot lower than it should be, and certainly in the past variants have not lived up to the threat they showed at lower point. [This is pretty cope-y. The data is incomplete, and JN.1 is now being asked to outcompete a variant mix that is now mostly varieties of BA.2.86, rather than a soup of slower-growing variants]
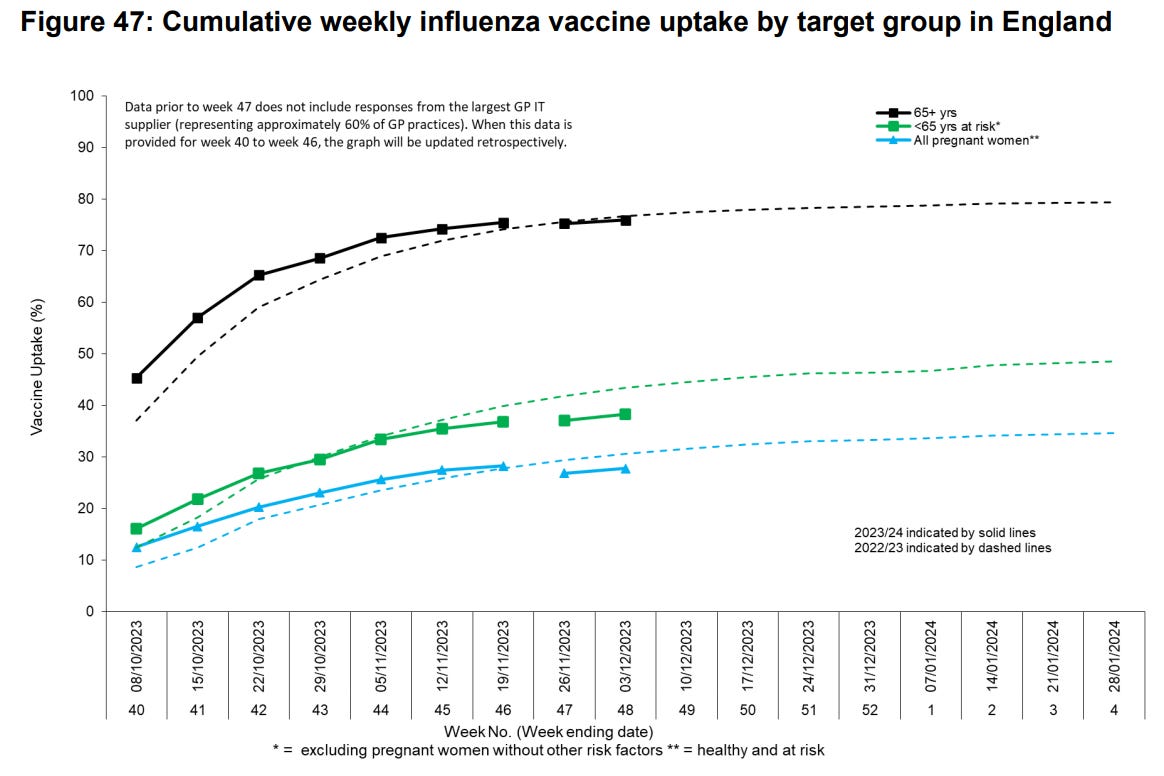
Finally, and - in terms of things that we can actually do now to avert this - vaccination for both flu and COVID is in fairly good shape. Around 70% of all those eligible for COVID boosters have taken it up, and this rises to 74% for those over the age of 75. And on flu vaccination, overall rates are in line with previous experience - for the youngest children it’s actually well ahead, while at-risk and pregnant women are just slipping behind last year.

If you’re looking for something to do personally, then pushing this “fairly good” to “very good” would be powerful. So do check whether you are eligible for any of these vaccinations, and do not put off your decision of whether you want to book in for one. However the next month or so plays out, time spent now to avoiding needing to be in an NHS hospital is pretty clearly time well spent.

Not crying wolf … unless there is a wolf
OK, so where are we (in the sense of: how much trouble are we in the UK and in particular, people who may need services of the NHS in the next few weeks.)
Bluntly, I think we’re in trouble.
First, a sizable COVID wave is nasty, but OK. We’ve had them before. This looks like another big one, certainly the worst we’ve seen this year, and up there with the ones in 2022. But we survived fine.
But now we add the second issue: this one is coming in the middle of winter, and quite possibly on top of a simultaneous flu wave. We have had that before as well, and we didn’t survive fine. It took one hour thirty minutes to get an ambulance for a stroke or heart attack. Some people didn’t survive at all.
Third, and possibly most damagingly is the fact that even before any of these things hit, the NHS is already showing huge strain. Ambulance trusts are already going to higher levels of crisis, delays are spiralling, incidents are being declared in hospitals, further surge beds are being opened up. And you just have to talk to people. That’s the system that is about to put under greatly increased pressure.
Add it all up, and you get a fairly clear picture:
This upcoming pressure appears likely enough and large enough to collapse NHS capacity - in particular its emergency medicine capacity - down to December 2022 levels or worse.
It is most likely to do this on or about the first two weeks in January 2024.
Alongside the various other pressures around that time (e.g., junior doctors’ strikes), I am hoping that the people who need to know about these little numerical projections, do know, have known for a while, and have their plans in place (e.g., delaying elective procedures) and ready to deploy. I hope they already know, I hope their plans are good, I hope they work.3
NB: This does not include the latest (incomplete) week of data - see below.
Is this a coincidence? Especially as it happened last year too? I would speculate that it isn’t, and that alongside variants, the seasonal factors which affect both transmission (temperature and humidity) and human behaviour (gathering indoors) are now affecting the transmission of both COVID and flu viruses in similar-enough ways, that we should not be surprised when their prevalence peaks at similar times.
In general, I tend to be sceptical of those who see doom and destruction in every new variant, upsurge or trend, but this time colour me worried.
In terms of personal action, then - as mentioned above - you can check whether you or loved-ones are eligible for flu shot/covid booster. Second, if there are people close to you who may need emergency medical care, it would be wise to come up with a plan for getting them to hospital that is independent of an ambulance responding in a timely manner. Call 111/999 as you normally would, and follow their advice, but do have an idea what you’d do if they told you that an ambulance would not be with you for a long time.