This winter in the UK - what to expect
It's out of the government's hands now

Over the next few months - from November 2023 to January 2024, the population of England and Wales will experience something that - though we’ve seen it before - remains utterly shocking for a Western, relatively rich country.
Anyone in England or Wales who feels a sudden intense chest pain with shortness of breath, or finds that they are slurring their words and half their body does not move, cannot expect an ambulance to arrive in a timely manner. They will be placed in ambulance priority Category 2 (in England, or Amber in Wales), and from there should consider themselves fairly lucky if the first emergency response vehicle arrives within an hour. They should still call 999 of course and follow the advice on the line, but anyone vulnerable enough to expect to need help would do well to make sure they have someone on standby to drive them to hospital. And if you break a leg, a hip, or an arm - best to find a good book. You’re likely to be categorised into Category 3, and the arrival of an ambulance within three hours would be worth a modest celebration.
As well as these most direct effects, there’s a second reason to care about ambulance responses, and in particular Category 2 times: they are a strong indicator on the overall pressure on NHS hospitals. Oversimplifying only a little: when wards are overfull, patients cannot be moved out of A&E, so patients cannot then be handed over from ambulances to A&E. Ambulances form a queue at the entrance, and are not available for the next 999 call. Category 1 calls are defined to contain only those patients who literally face death within minutes, the whole system (rightly) acts to protect them at all costs, so system delays are passed to Category 2, and therefore these times then become diagnostic of the capacity of the whole system.
So, if you track Category 2 times over the last few years, you can follow the extent that - due a combination of long-term underinvestment, a lack of personnel, and COVID pressure - emergency medicine in the NHS has been falling apart.
Compared to the target of 18 minutes, the actual Category 2 times have looked like this:

Last winter (2022-3) this appalling situation finally did what it had been warning it could do for months - and blew up: a combined flu, RSV and COVID wave all hit an NHS already on its knees. And so we saw the near-incredible state of a person in the South West region calling an ambulance for a heart attack or stroke having an expected wait of 2 hours and 30 minutes. If they were less lucky (i.e., they were in the 10% more “disappointing” times in December) their waiting time was 6 hours 39 minutes.1
Now, according to the NHS’ official spokespeople, this situation is nothing to worry about. Even after December 2022, they have been consistently and firmly asserting that they see no link between the capacity crunch and the national excess death measures that shot up to +30% at the same time. Not quite the peaks we saw in the pandemic, but dramatic and deadly nonetheless.2

And since that December, flu and RSV have vanished, and COVID has plummeted. Response time have also recovered somewhat, although the NHS charter 18 minutes target remains well out of reach.
It’s noticeable that as these numbers have improved excess death numbers have also receded to a much lower rate (though this is obscured by registration delays, which I’ve written about before).
The big question: will it get as bad this winter?
Our current national situation - as compared to previous years, looks like this:

So despite a warm, largely pleasant September and October our trajectory is closer to 2021 and 2022 than it is previous years. Whatever package of reforms the government and NHS leadership have been proudly announcing (several times over), they do not appear to have worked, in the sense that we are nowhere near returning to even vaguely acceptable response times.
For a more “inside baseball” view, we can look directly at the handover times (=waiting times of ambulances to hand over patients at A&E). The target for this is 15 minutes, and it looks like this:
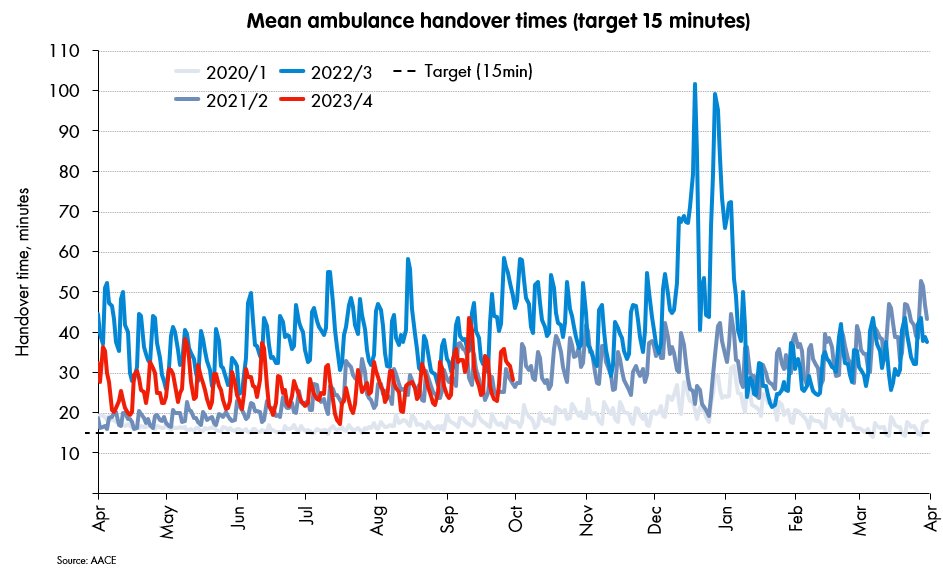
Again, this year’s performance is tracking 2021/2, and occasionally flipping up to 2022/3. Each ambulance is losing around 15 minutes of capacity vs target for every patient handed over to hospital - again, the message appears clear: whatever the spin, the core issues have absolutely not been addressed.3 And I think we can now call it: in 2023/4 we’re looking at either a repeat of 2021/2 (scary) or of 2022/23 (deadly).
In addition, we can also be clear that the overwhelming factor that determines whether we’re looking at “scary” or “deadly” is now pretty much out of the government and NHS management’s hands.4 It is down to how bad respiratory diseases are in December, and in particular, what kind of a flu wave we get.
How to break a health service
We can look at a picture of how these came together (approximate and incomplete, but perhaps helpful) - using a mix of data from the UKHSA influenza report, the coronavirus dashboard, and the new respiratory data dashboard.5

In December 2020 we were hit by a remarkably high COVID spike - quite possibly the deadliest of all, but were otherwise in lockdown, with no flu at all. The NHS was put onto a war footing, and survived (though the mental wellbeing of some medics did not, and they left the service shortly after).
In December 2021, we were hit by the first Omicron wave (far higher infections, much lower admissions) and again nothing else. In particular, again, there was no flu. And the NHS survived.
In December 2022, we were hit by a triple-whammy: a fair amount of COVID, a fair bit of RSV, plus a short and intense flu spike … and emergency care broke.
That is, the 2022/3 spike was the first we had since the start of COVID where there was a normal winter respiratory disease one (RSV and flu). And it’s worth noticing that while it was very intense, it was not a particularly deadly flu seasons (compare to 2017/18 for example). But on top of a COVID and RSV spike (RSV hits children, COVID and flu older people), even this short, sharp flu season was enough to break the whole thing.
Despite government rhetoric, there’s nothing I can see in the latest numbers that suggests we have a more robust system this time around. So it’s down to demand.
COVID appears to be peaking for the moment, which is good news - we can expect this to be lower. RSV is already rising fast, and the 2022 peak looks very within reach. So it looks like it’s down to the flu.
Please get your flu shot, stay safe, and let’s see how we do.
Not a typo. Six hours and thirty-nine minutes. I’ve checked it eight times now.
Of course, the causation almost certainly goes in both directions in a loop: the flu, RSV and COVID wave contributed to the pressure on hospitals, and the pressure on hospitals almost certainly contributed to the death toll. But the NHS spokespeople (and leadership) wibbling about ageing populations is disingenuous at best. There’s a connection, it’s a strong one, and they just sound absurd trying to deny it.
The observant will also note the temporary plummet in the middle of December 2022. These are the day of the ambulance strikes - it’s not fully clear what the reported times mean here, but they jump back to the worst state after Christmas.
To state the bleedin’ obvious: even Rishi Sunak’s revised target of getting back to a mean of 30 minutes “over the course of the year” will be missed by miles. It was set to be easily achievable to chalk up a “victory”, and there’s absolutely zero chance of hitting it. A total failure of technocratic government and planning, and it’s noticeable that - for example - Rishi Sunak hasn’t mentioned it for a while. More puzzlingly, no interviewer has either.
In particular, the flu numbers are back-of-envelope: derived from the ICU rates, scaled to a ratio to SARI-Watch admission estimates for 2022 onwards. Don’t trust these too far.